Background
Human digestion is a complicated network of hollow organs. The stomach is the most important organ for food digestion out of all of them. Several hazardous stimuli, including alcohol, reflux bile salt, and hydrochloric acid, are not easily absorbed by the stomach. The stomach has many defines mechanisms that contribute to its high tolerance to harmful chemicals. Peptic ulcers, however, result when harmful reasons take precedence over these protective measures. An erosion in the gastrointestinal mucosa's pepsin- and acid-saturated lining is indicative of peptic ulcer disease. 10% of people worldwide suffer from gastric ulcer disease, the most common gastrointestinal ailment.1
The population suffer from peptic ulcers or other symptoms bad enough to need medical attention. The two most significant illnesses that are medically necessary are reflux disease of the stomach and ulcers. More than 4 million Americans suffer from duodenal and stomach ulcers; each year, 350 000 new cases are reported; 180 000 patients are admitted to hospitals to receive treatment; 5,000 of these individuals pass away as a result of their ulcers. In the United States, the lifetime risk of developing a peptic ulcer is 4% for women and about 10% for men.2 An imbalance between mucosal protective forces and stomach aggressive factors appears to be the aetiology of peptic ulcers. Peptic ulcers are caused by the pepsinogen generated by parietal cells; these ulcers can be categorized as stomach, duodenal, or oesophageal based on where they manifest. The development of gastric ulcers can be influenced by both aggressive and defensive factors, such as endogenous protective chemicals, blood supply, mucosal production, and the gut barrier. 3 Hematemesis, a symptom of chronic UGI bleeding, has been linked to a peptic ulcer risk factor. Hematemesis is described by the vomiting of digested food (melena), blood, and a substance like coffee grounds. The nasogastric tube lavage used to diagnose upper gastrointestinal (UGI) disease contains either blood or something like coffee. For most bleeding ulcer patients, a combination of endoscopic surgery, medication therapy, and fluid and blood transfusion is the best course of treatment. Perforation: In the small, middle, and large intestines, ulcers account for 60, 40, and 20% of perforations, respectively. The term "ulcer penetration" refers to the process by which an ulcer breaks down partially away from the colon's wall and filters all of its contents into the peritoneal cavity. According to the surgical treatment regimen, 20% of ulcers had permeation; however, just a small proportion of these ulcers would have clinical significance. Weight loss, diarrhoea, and acidic irritation are typical signs of these problems. Watery vomit is an uncommon but warning symptom.
There isn't enough reliable clinical data to support the suggested course of treatment for superficial ulcers. Obstruction: One of the most typical symptoms of ulcers is the occlusion of the stomach wall. Duodenal or pyloric section ulcerations constitute the majority of cases, which affect 5% of patient populations. Modifications to diet and lifestyle: The therapy of peptic ulcers may be complicated by aspirin and similar NSAIDs (non-steroidal anti-inflammatory drugs), alcohol, coffee, including decaf, tea, and other substances. Smoking prolongs the healing process of ulcers. Researchers have found that those who have symptoms of ulcers consume higher amounts of carbs than people who do not. It has also been observed that sugar increases stomach pH. The stomach and intestines may become irritated by salt. People who consume excessive amounts of salt have been found to have a greater likelihood of stomach ulcers when certain amino acids are consumed. Glutamate is the essential energy source in the cells lining the stomach and intestine. 4
Types of Peptic Ulcer 5
Peptic ulcers can be classified into several types based on their location and underlying causes.
Gastric ulcers: These ulcers occur in the lining of the stomach. They are often associated with Helicobacter pylori infection or the use of NSAIDs. Gastric ulcers can cause symptoms such as abdominal pain, bloating, and nausea.
Duodenal ulcers: Duodenal ulcers form in the upper part of the small intestine called the duodenum. They are more common than gastric ulcers and are also linked to H. pylori infection and NSAID use. Symptoms of duodenal ulcers may include abdominal pain, especially between meals and at night, along with bloating and heartburn.
Esophageal ulcers: These ulcers develop in the lining of the esophagus, often due to gastroesophageal reflux disease (GERD) or excessive alcohol consumption. They can cause symptoms such as chest pain, difficulty swallowing, and heartburn.
Stress ulcers: These ulcers are related to severe physical stress or trauma, such as major surgery, severe burns, or critical illness. Stress ulcers can occur in the stomach (stress-related mucosal damage) or the duodenum and are typically managed in hospitalized patients.
Refractory ulcers: Refractory ulcers are those that do not heal despite appropriate treatment, such as medication to reduce stomach acid and eradicate H. pylori.
Physiological factors associated with gastric ulcer: 6, 7, 8, 9
The epithelium of the stomach gets damaged by chemical or H. pylori gastritis, which is nearly always present in association with gastric ulcers. The majority of gastric ulcer patients produce less acid than those who have duodenal ulcers and even less than those who are healthy. There are the following components involved: Acid back diffusion into the mucosa; a decrease in the bulk of parietal cells; issues with the parietal cells themselves. Patients with gastric ulcers rarely experience excessive acid output. Usually, these people have duodenal ulcers that are situated around the pylorus. The hypersecretion of gastric juices associated with Zollinger-Ellison's syndrome is linked to severe duodenal and jejunal ulceration, not stomach ulcers as is more commonly the case.
Treatment approaches for gastric ulcer
Drugs that decrease the production of acid. Acid blockers, also known as histamine (H-2) blockers, limit the production of stomach acid in the digestive tract, which eases the pain of ulcers and speeds up their recovery. An antacid is a fast-acting analgesic that also mitigates any stomach acid that may be present. As a side effect, diarrhoea or constipation could occur, depending on the underlying substances. 10
Regulation of Acid Secretion
The parietal cells in the stomach secrete roughly two litres of hydrochloric acid daily. This acid facilitates digestion by killing germs and increasing the solubility of food. The ideal pH range of 1.8 to 3.5 must be reached for the digestive enzyme pepsin to operate as intended. An essential protein for the synthesis of acids (or proton pump) is H+ /K + -ATPase. This protein uses the energy from ATP hydrolysis to pump hydrogen ions into the lumen in exchange for potassium ions. Acid secretion is triggered by the H+/K+-ATP ases’s migration to the parietal cell's apical membrane. H+/K+-ATPases are present in vesicles within a cell while it is at rest (not activated). When the cell is active, these vesicles attach to the plasma membrane, expanding its surface area and the quantity of proton pumps therein. Three regulatory molecules—acetylcholine, histamine, and gastrin—encourage the production of acids, while somatostatin, the fourth regulatory molecule, inhibits the secretion of acids. Acetylcholine is a neurotransmitter released by enteric neurons. Histamine is a paracrine substance that is released by enterochromaffin-like (ECL) cells. G cells, endocrine cells located in the stomach epithelium, release the hormone gastrin. Somatostatin, a paracrine or hormone, is also released by the endocrine cells of the stomach epithelium. The illustration shows how interaction between the positive and negative regulators encourages acid secretion. The amount of acid released by parietal cells is directly increased by histamine and acetylcholine. Gastrin promotes the release of histamine from ECL cells, which raises the generation of acid. Furthermore, gastrin stimulates the growth of parietal cells directly. The production of somatostatin is increased when the stomach's pH is too low. By directly controlling parietal cells and blocking the release of histamine and gastrin, the positive regulators, somatostatin lowers acid secretion. As food is consumed and moves through the different parts of the upper GI tract, the balance of activity between the various regulators shifts.
Antioxidant activity refers to the ability of substances to neutralize or inhibit the harmful effects of free radicals and reactive oxygen species (ROS), which are highly reactive molecules that can cause oxidative stress and damage to cells, proteins, lipids, and DNA. Oxidative stress is implicated in various diseases, including cancer, cardiovascular disorders, neurodegenerative conditions, and aging. Antioxidants, both enzymatic and non-enzymatic, counteract oxidative damage by donating electrons to stabilize free radicals. Research into antioxidant activity is crucial for identifying natural and synthetic compounds that can mitigate oxidative stress and improve health outcomes. This paper explores the mechanisms of antioxidant action, the methods used to measure antioxidant activity, and the potential therapeutic applications of antioxidants in disease prevention and treatment. 11 This plant is widely distributed throughout the tropical and subtropical region of Karnataka state. The Senegalia chundra plant belongs to the family Fabaceae and genus senegalia. Its bio compounds were exhibiting various clinical importance. This plant called as Tare Gida, Kachu, Kadhira, Kempu jali in Kannada, Karingali in Malayalam, Khair in Marathi and Sundra in Telugu. The plant contains various secondary metabolites like flavonoids, tannins, alkaloids, triterpenoids, cardiac glycosides, sesquiterpene’s and essential oil. The traditional uses include: treating diarrhea, Astringent, bactericide etc.12
The ulcer protective effects of Baccharis trimera DC, Solidago chilensis, Cordia dichotoma plants have similar phytoconstituents ( Ketan Vinayakrao etal.,) as Senegalia chundra, by taking these plants as reference the research is conducted.

Table 1
Shows the pharmacological properties
Materials and Methods
Experimental animals
Healthy Wistar albino rats of either sex weighting between 180-250g were taken for the studies. were used for the experiment. Each rat was housed in a plastic box cage under standard conditions at 19–25°C and was kept under 12/12 h light/dark cycle. The rats were allowed free access to standard pellet feed and water ad libitum. The study was carried out according to the Use of Laboratory Animals and Organization of Economic Co-operation and Development (OECD) guide lines.
Plant collection and authentication
The fresh bark of Senegalia chundra was collected from the hill of the Veerapura Village of Haveri district Hirekerur taluk. The plant was authenticated by taxonomist Dr. Haleshi Asst. Professor at Davangere university, and dried under shed in Bapuji Pharmacy college, Davangere, Karnataka, India.
Preparation of the extract
The coarse powdered material was subjected to Soxhlet extraction with ethanol (95%). The temperature (70-80°C) was maintained on an electrical heating mantel with thermostat control. Appearance of Golden yellow colored solvent in the siphon tube was taken as the end point of extraction. The ethanolic extract was evaporate to dryness and extract was concentrated to get powdered form and preserved in the desiccator. The obtained extract was subjected to phytochemical investigation, antioxidant and pharmacological activities.
Evaluation of Antioxidant Activity by In-Vitro Method
Principle of DPPH (α, α-diphenyl-β-picryl hydrazyl) 15, 16
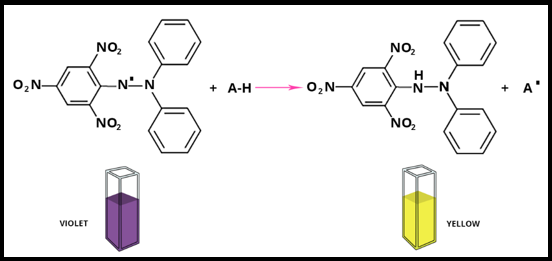
The DPPH (2,2-diphenyl-1-picrylhydrazyl) assay is a widely used method to evaluate the antioxidant activity of compounds by measuring their ability to donate electrons or hydrogen atoms to neutralize free radicals. The principle is based on the reduction of the DPPH radical, a stable free radical with a characteristic deep violet color, into a colorless or pale-yellow compound in the presence of an antioxidant. The decrease in absorbance at 520 nm, due to the scavenging of the DPPH radical by an antioxidant, is measured spectrophotometrically.
Free Radical Scavenging Effect: 17
The inhibition-based in vitro approaches are used. Samples are added to a free radical scavenging system, the free radical action is evaluated, and the inhibition is related to the sample's antioxidant activity. The generated radical, the reproducibility of the creation procedure, and the end point employed for the determination differ substantially amongst methods.
Procedure
DPPH preparation
Reagent 2, 2-diphenyl 1-picryl hydrazyl solution (DPPH,0.1mM): 4mg of DPPH was dissolved in 100 ml of methanol.
Preparation of standard solutions: (Stock) Ascorbic acid (100mg) is dissolved in 100ml of freshly distilled Methanol which gives 1000 µg/ml concentration. Prepare a different concentration of 50, 100, 200, 400, 600 µg from above stock. Add 0.5, 1, 2, 4, 6 ml from the stock solution (1000 µg/mL) to the 10 ml Volumetric flask. And add 3ml of DPPH Solution to the above 10 ml volumetric flask which contains standard solution, made up to the mark with methanol.
Preparation of Ethanolic Extract of Senegalia Chundra Bark Solutions
Senegalia chundra (100mg) is dissolved in 100ml of freshly distilled Methanol which gives 1000 µg/ml concentration. Prepare a different concentration of 50, 100, 200, 400, 600 µg/ml from above stock. Add 0.5, 1, 2, 4, 6 ml from the stock solution (1000 µg/mL) to the 10 ml Volumetric flask. And add 3ml of DPPH Solution to the above 10 ml volumetric flask which contains standard solution, made up to the mark with methanol. Prepare a control by adding 3ml of DPPH and add methanol solvent. Blank Methanol. Incubation period of 30min was allowed at room temperature in dark place to complete any reaction that is to be occurred. Then absorbance was measured by UV spectrophotometer at λ max 520 nm against blank. Ascorbic acid used as standard free radical scavenger activity of extract was compared with it. Activity of the sample was calculated by the formula.
Acute oral toxicity studies:18
The acute oral toxicity study of the ethanolic extract of Senegalia chundra bark was conducted in Swiss albino mice to assess its safety profile. The test was performed according to OECD guidelines 423 for acute oral toxicity.
Grouping and dosing of animals
Animals were randomly assigned to different groups each consisting of six rats.
Pylorus ligation model19, 20, 21, 22, 23, 24
Healthy Wistar albino rats of either sex weighting between 180-250g were taken for the studies. The animals were divided in five groups (each group contain 6 animals).
Group I – Normal, Group II (Control) – Animals treated with Normal saline (0.9%) 1ml/rat orally for 7 days, Group III – Animals treated with Standard Lansoprazole (20 mg/kg) orally for 7 days, Group IV – Animals treated with extract of Lower dose of Senegalia chundra (200 mg/kg) orally for 7 days, Group V - Animals treated with extract of Higher dose of Senegalia chundra (400 mg/kg) orally for 7 days.
Indomethacin induced gastric ulcers25, 26, 27, 28
Healthy Wistar albino rats of either sex weighting between 180-250g were taken for the studies. The animals were divided in five groups (each contain 6 animals).
Group I – Normal, Group II (Control) – Animals treated with 30mg/kg body weight of indomethacin, Group III – Animals treated with Standard Lansoprazole (20mg/kg), Group IV – Animals treated with extract of Lower dose of Senegalia chundra (200mg/kg) + indomethacin (30mg/kg), Group V - Animals treated with extract of Senegalia chundra Higher dose of (400mg/kg) + indomethacin (30mg/kg) for 21 days.
Anti-Ulcer Activity Evaluation
Pyloric ligation-induced ulcer model
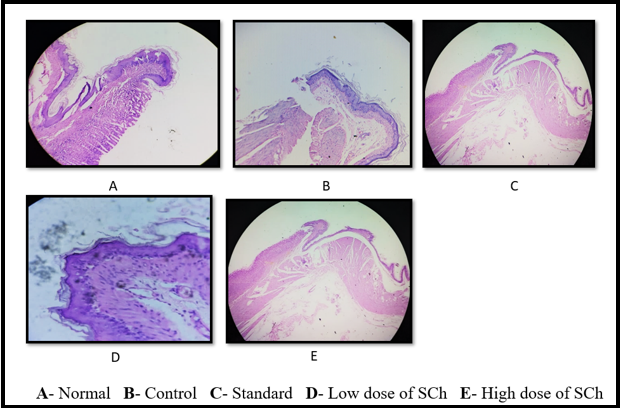
The rats were subjected to pyloric ligation according to the method of Shay et al., with some modifications. In the pyloric ligation process the rats were fasted for 24 h before pylorus ligation with water ad libitum. Normal saline (1ml/rat,orally) were administered daily to all the animals during fasting period. Animals were anaesthetized; the abdomen was opened by midline incision below the abdomen. The pyloric portion of the stomach was slightly lifted out and ligated, avoiding damage to its blood supply. The stomach was placed back carefully and the abdominal muscular and skin layers were closed with sutures. Animals were sacrificed 5 h after pylorus ligation. The rat stomach was removed and opened along the greater curvature and then washed with physiological solution (0.9% w/v NaCl). Gastric content was subjected to measurement of gastric volume, free acidity and total acidity. Moreover, isolated tissue was employed for the measurement of ulcerative index and microscopic features.
Macroscopic evaluation of stomachs
The stomachs were opened along the greater curvature and rinsed with saline to remove gastric contents and blood clots and examined by a 10× magnifier lens to assess the formation of ulcers. The number of ulcers was counted. Scoring of ulcers was made as follows:
Ulcer-index were determined by following the scoring method: 0= No ulcer, 1= Superficial ulcers 2= Deep ulcers, 3= Perforation, mean ulcer score for each animal is expressed as Ulcer Index.
The percentage of ulcer protection were determined.
Volume of gastric juice
Gastric content was evacuated into graduated tube by cutting along the greater curvature of the stomach, and the gastric volume is directly read from the graduation tubes.
Total acidity and free acidity
It is based on simple acid-base titration. Gastric juice (1mL) was pipette into a 100 mL conical flask and diluted with 9 mL distilled water. Two or three drops of Topfer’s reagent is added and titrated with 0.01 N sodium hydroxide until all traces of red color disappeared and the colour of the solution was yellowish-orange. The volume of alkali added was noted. This volume corresponds to free acidity. Two or three drops of phenolphthalein was then added and the titration was continued until a definite red ting appeared; the volume of alkali added was noted. The volume corresponds to total acidity, Acidity was expressed in terms of mEq/L.
Indomethacin Induced Gastric Ulcers
The study was carried out using an acute model with indomethacin induced ulcers. The rats were kept fasting for 24 h before the experiment with free access to water ad libitum. Except for the healthy group, all the groups were administered indomethacin 30 mg/kg body weight on 21st day. Then on the next day, all animals were sacrificed by anesthesia and subjected to respective parameters estimation. Ulcer-index was determined by following the scoring method: 0= No ulcer, 1= Superficial ulcers 2= Deep ulcers, 3= Perforation, mean ulcer score for each animal is expressed as Ulcer Index and the percentage of ulcer protection was determined.
Data were expressed as mean ± standard error of mean and statistically evaluated using one-way analysis of variance, followed by Tukey’s multiple comparison tests using Graph Pad Prism 5 software.
Results
Anti-oxidant activity
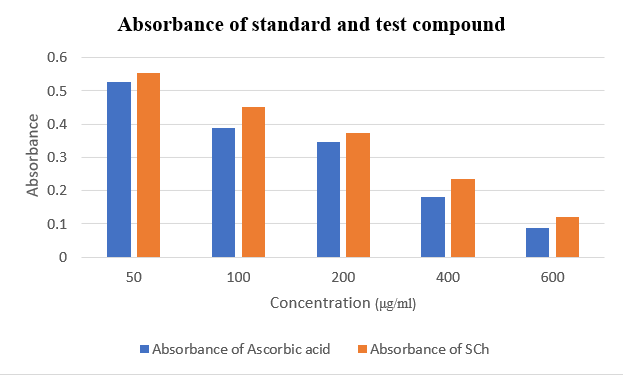
Free radicals are constantly produced, causing substantial damage to tissue and bio molecules, which can lead to a variety of diseases. Senegalia chundra extract is used as an alternative source of medicine to treat oxidative stress-related diseases. The antioxidant activity of Bark portion of Senegalia chundra (SCh) extract was evaluated using the DPPH method in this work. At a concentration of 600 μg/ml, an ethanolic extract of Senegalia chundra Bark showed strong DPPH radical inhibition (93.59 %). In a DPPH in-vitro experiment, sequentially produced Et-OH extracts revealed high antioxidant activity.
Table 3
Antioxidant activity of Bark part of Senegalia chundra by DPPH method.
Ulcer Protective Activity
Pylorus ligated ulceration model
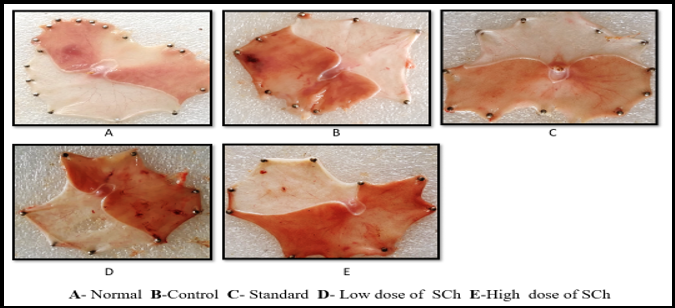
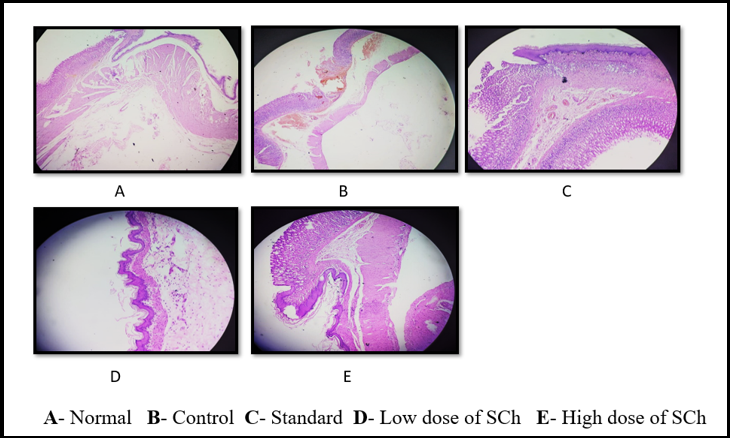
Table 4
Results of ulcer protective activity in pylorus ligated ulceration
Indomethacin Induced Ulceration Model
Results of ulcer protective activity in indomethacin induced ulceration
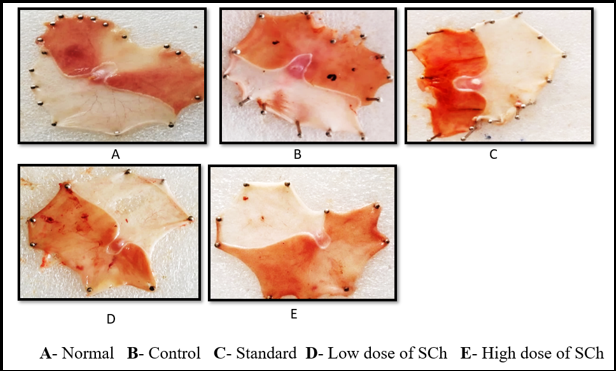
Table 0
Discussion
This study aimed to evaluate the ulcer-protective and antioxidant properties of Senegalia chundra bark, focusing on its effects on pylorus ligation and indomethacin-induced ulcerations. The bark was collected, dried, and extracted using ethanol. The resulting extract was evaluated for its antioxidant properties, including flavonoids, alkaloids, glycosides, and tannins. The DPPH assay showed significant antioxidant activity, with the extract effectively neutralizing free radicals and achieving a substantial inhibition of 87.12% at a concentration of 600 µg/ml. The acute toxicity studies on Swiss albino mice demonstrated the extract's safety for use at doses up to 2000 mg/kg. The study also found that rats subjected to pylorus ligation and Indomethacin exhibited significant morphological aberrations in the gastric tissue. Treatment with Senegalia chundra extract resulted in a significant reduction of these ulcerations, comparable to that achieved with Lansoprazole, a recognized standard in ulcer prevention and treatment. These findings highlight the potential efficacy of Senegalia chundra extract as a therapeutic agent in managing gastric ulcers.
In the research on the ulcer protective effects of Baccharis trimera DC, the presence of key phytoconstituents such as flavonoids, alkaloids, tannins, glycosides, has been identified, which are known for their ulcer-protective properties. Similarly, the study on the ulcer protective effect of Solidago chilensis against drug-induced ulcerations in mice also highlights the presence of similar bioactive compounds, including flavonoids, and tannins. The anti-ulcer agents: from plant extracts to phytochemicals in healing promotion (Mehdi SR et al., 2018) article provides strong evidence that these phytoconstituents have proven ulcer protective activities, reinforcing the therapeutic potential of Senegalia chundra. The presence of these phytochemicals in both plants suggests that the ulcer protective effects of Senegalia chundra could be attributed to similar mechanisms, supporting its use in ulcer protection.
Conclusion
The study found that Senegalia chundra bark has potential as an antioxidant and ulcer-protective agent. It contains flavonoids, alkaloids, and tannins, which support its medicinal potential. The extract's antioxidant activity is equivalent to ascorbic acid, and it effectively prevents ulcers. Histological investigation confirmed the extract's effectiveness, suggesting its potential as a natural therapeutic agent for stomach ulcers.